Topical Steroid Potency Chart: Minimizing Skin Side Effects
 Jun, 6 2026
Jun, 6 2026
Topical Steroid Safety & Usage Calculator
Treatment Parameters
Safety Assessment & Guidelines
Enter your details to see safety limits and dosage instructions.
Itchy, red, and inflamed skin is miserable. Most of us reach for a tube of cream to stop the itch, but not all creams are created equal. Using the wrong strength of topical corticosteroids is medications applied to the skin to reduce inflammation and immune response can lead to thinning skin, visible veins, or even systemic health issues. The key to safe treatment isn't just picking a brand; it's understanding the potency class.
Think of topical steroids like volume knobs on a stereo. You wouldn’t blast the music at maximum volume for a quiet conversation, right? Similarly, you shouldn’t use the strongest medical-grade steroid for a mild rash on your face. A clear understanding of the potency chart is a standardized classification system that ranks steroids from least to most potent helps you match the right medicine to the right problem. This guide breaks down how these charts work, which classes are safe for where, and how to minimize the risk of serious side effects.
Understanding the Seven-Class Potency System
In the United States, the Food and Drug Administration (FDA) established a seven-class system in 1997 to standardize how doctors prescribe these drugs. Class I represents the "superpotent" steroids, while Class VII contains the mildest options. This system exists because potency varies wildly between different molecules and concentrations.
Potency isn't random. It’s determined by three main factors: the molecular structure of the steroid (which accounts for about 60% of its strength), the concentration of the active ingredient (25%), and the vehicle or base it comes in, such as an ointment or cream (15%). Ointments, for instance, allow for 15-20% higher absorption than creams because they create a better seal over the skin. Understanding this hierarchy is crucial for safety.
| Class | Potency Level | Common Examples | Typical Use Cases |
|---|---|---|---|
| I | Superpotent | Clobetasol propionate 0.05%, Halobetasol propionate | Severe plaque psoriasis, thickened skin |
| II - III | High Potency | Betamethasone dipropionate, Mometasone furoate | Moderate eczema, lichen simplex chronicus |
| IV - V | Moderate Potency | Triamcinolone acetonide, Fluocinolone acetonide | Mild-to-moderate eczema on body |
| VI - VII | Low/Mild Potency | Hydrocortisone 0.1-2.5%, Desonide | Facial rashes, diaper dermatitis, sensitive areas |
The difference between Class I and Class VII is massive. Clobetasol propionate 0.05%, a Class I steroid, is significantly stronger than hydrocortisone 1%, a Class VII option. Using a Class I steroid on delicate facial skin is like using a sledgehammer to crack a nut-it works, but it causes unnecessary damage.
Why Location Matters: Skin Thickness and Absorption
Your skin is not uniform. The thickness of your skin changes depending on where you look, and this directly impacts how much steroid your body absorbs. This is why the same tube of cream might be safe on your elbow but dangerous on your eyelid.
Skin in intertriginous areas-places where skin folds against skin, like the groin, armpits, or under the breasts-is much thinner. In these spots, potency effectively increases by one class. A moderate steroid applied here acts like a high-potency one. Conversely, the skin on your palms and soles is very thick. Steroids penetrate poorly there, often requiring higher potency to be effective.
Facial skin is particularly vulnerable. Studies show that applying mild potency steroids (Class VI-VII) to facial eczema reduces the risk of skin atrophy (thinning) by 65% compared to using moderate potency (Class IV-V). Yet, surveys indicate that 42% of patients inadvertently apply moderate-to-high potency steroids to their faces, increasing their side effect risk fourfold. Always default to the lowest effective potency for the face, neck, and genitals.
Minimizing Side Effects: Time and Quantity
Even the correct steroid can cause harm if used incorrectly. The two biggest mistakes patients make are using too much product and using it for too long. These errors lead to conditions like telangiectasia (visible broken blood vessels), striae (stretch marks), and topical steroid withdrawal.
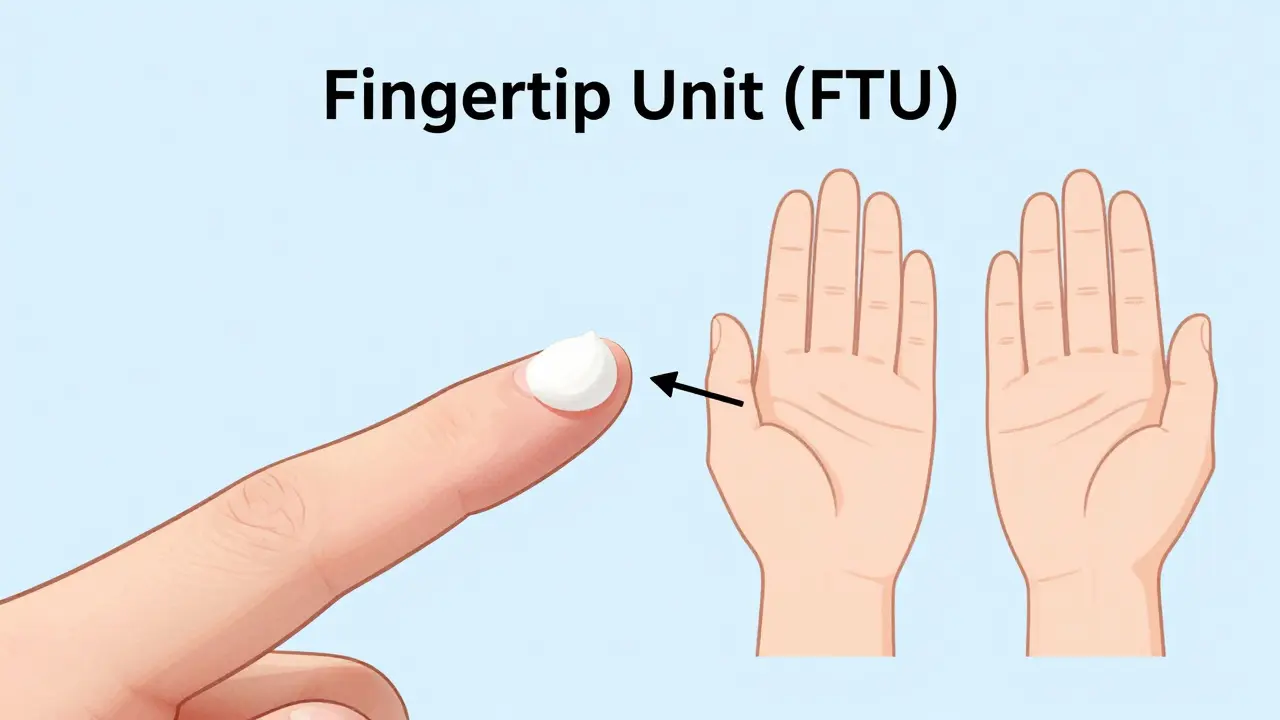
To control quantity, use the "fingertip unit" (FTU) method. One FTU is the amount of cream squeezed from the tip of an adult finger to the first crease. This small amount covers an area equivalent to two adult palms. Research shows that 35% of patients use two to three times the recommended amount, which drastically increases systemic absorption without improving results.
Duration is equally critical. The American Academy of Family Physicians strongly recommends against continuous use of ultra-high-potency steroids (Class I-II) for more than three weeks. For low-to-high potency steroids, the limit is generally three months. Prolonged use suppresses the local immune system and can damage collagen fibers in the skin.
- Limit Continuous Use: Do not use superpotent steroids continuously for more than 2-3 weeks unless directed by a specialist.
- Use Proactive Therapy: For maintenance, switch to a mild steroid applied twice weekly to previously affected areas. This strategy reduces eczema flares by 68% over 16 weeks compared to stopping treatment entirely.
- Avoid Occlusion Unless Prescribed: Covering treated skin with plastic wrap increases absorption significantly. Only do this if your doctor explicitly instructs you to, as it raises the risk of side effects.
Special Considerations for Children
Children are not just small adults. Their skin has a higher surface-area-to-body-weight ratio, meaning they absorb up to three to five times more medication per pound of body weight than adults. This makes them significantly more vulnerable to systemic side effects, including HPA axis suppression, which affects hormone production.
Data from the Pediatric Dermatology Registry indicates that 8.7% of children improperly treated with high-potency steroids developed hormonal issues. To mitigate this, the American Academy of Pediatrics mandates reducing standard adult doses by 50-75% for children under 12. Furthermore, treatment duration should be strictly limited to 7-14 days for moderate potency steroids. Always consult a pediatrician before starting any steroid regimen for a child, and avoid using anything stronger than Class VI on young children unless absolutely necessary.
Modern Tools and Future Trends
The landscape of steroid management is evolving. In 2022, the FDA required all prescription topical steroids to include potency classification on their labels, aiming to reduce confusion. Before this, many patients didn't know how strong their medication was. Now, seeing "Class II" on the box provides immediate context.
Digital tools are also stepping in to help. The American Academy of Dermatology Association released an updated digital potency tool in 2023 that uses AI to recommend treatments based on patient-specific factors like age and body site. Early trials showed this reduced medication errors by 32%. Additionally, new non-steroidal alternatives like crisaborole and ruxolitinib are becoming more common, offering relief without the risk of skin thinning, though they may take longer to show full results.
As we move forward, expect to see more "potency-adjusted" formulations designed to deliver targeted relief with fewer side effects. However, until those become standard, mastering the current potency chart remains your best defense against skin damage.
What is the safest topical steroid for the face?
The safest topical steroids for the face are those in Class VI and VII, such as hydrocortisone 1% or desonide. These mild potency steroids carry the lowest risk of causing skin thinning or visible blood vessels when used short-term.
How long can I use a Class I steroid like clobetasol?
You should generally not use Class I superpotent steroids continuously for more than two to three weeks. Prolonged use significantly increases the risk of permanent skin damage and systemic absorption. Always follow your doctor's specific timeline.
What is a fingertip unit (FTU)?
A fingertip unit is the amount of cream squeezed from the tip of an adult index finger to the first joint. One FTU equals approximately 0.5 grams of cream and covers an area the size of two adult palms. Using this measure prevents over-application.
Are ointments stronger than creams?
Yes, ointments typically allow for 15-20% higher absorption than creams because they are oil-based and provide better occlusion. This means the same potency steroid will act more strongly in an ointment form.
Can topical steroids affect my hormones?
Yes, especially in children or when large amounts of high-potency steroids are used over large areas for extended periods. This can lead to HPA axis suppression, interfering with natural cortisol production. Limiting duration and potency minimizes this risk.