Psoriatic Arthritis: Understanding the Link Between Skin and Joint Inflammation
 Apr, 29 2026
Apr, 29 2026
Imagine waking up with joints that feel like they've been rusted shut, only to notice a new patch of scaly, red skin on your elbow. For many, this isn't just a coincidence; it's the calling card of Psoriatic Arthritis is a chronic autoimmune condition where the immune system attacks both the joints and the skin. It affects roughly 1 to 2 million Americans, typically hitting between the ages of 30 and 50. While it's often seen as a "skin problem" that turns into a "joint problem," the reality is more complex. About 15% of people actually feel the joint pain before any skin rash ever appears, which is why so many people struggle to get a correct diagnosis for years.
The Skin-Joint Connection: How It Happens
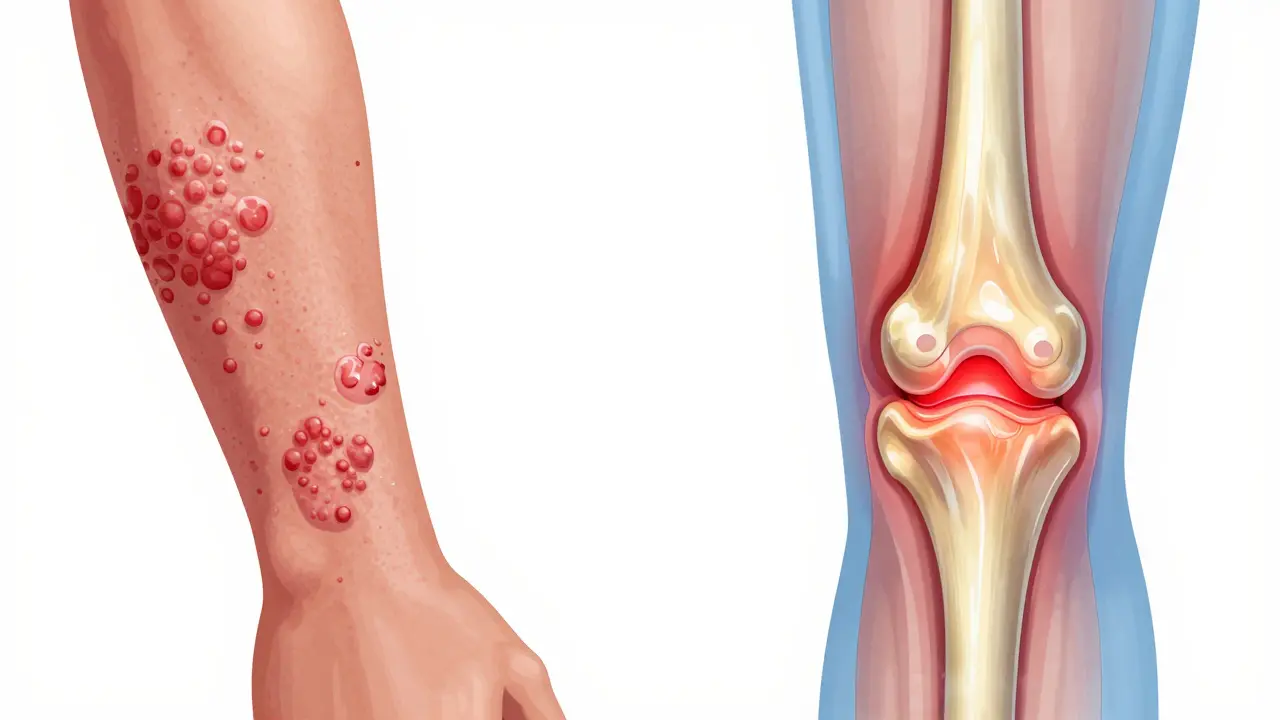
To understand why your skin and joints are both acting up, you have to look at the immune system. In a healthy body, your immune system fights off viruses. In someone with this condition, the system gets confused. It starts attacking the synovium (the lining of your joints) and the entheses (the spots where tendons and ligaments attach to bone). Because the same inflammatory pathways are active in both the skin and the joints, a flare-up in one often mirrors a flare-up in the other.
Most people with this condition start with Plaque Psoriasis is the most common form of the disease, characterized by raised, red patches covered with silvery scales . If you have this and start feeling stiffness in your fingers or a dull ache in your lower back, your body is sending a signal that the inflammation has moved deeper into your musculoskeletal system.
Spotting the Warning Signs
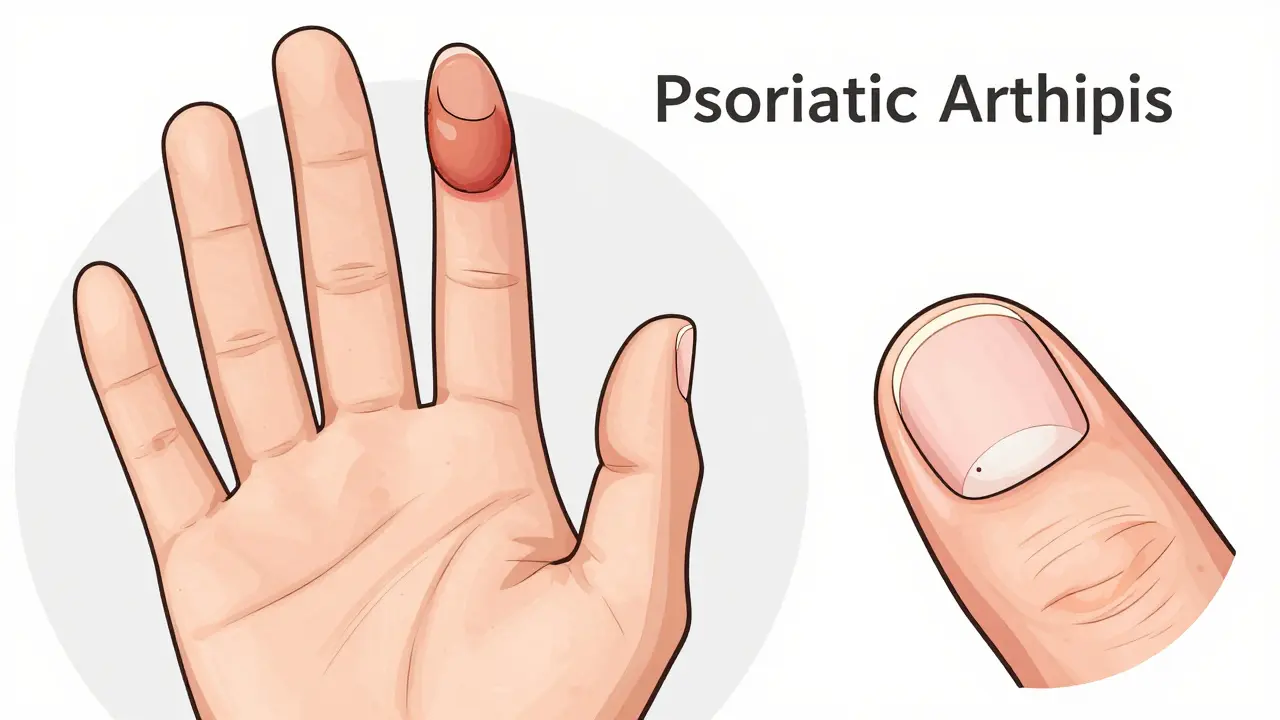
Psoriatic arthritis doesn't look like every other kind of joint pain. It has a few "signature" moves that help doctors tell it apart from things like rheumatoid arthritis. One of the most distinct is Dactylitis is the swelling of an entire finger or toe, making it look like a small sausage . This happens in 40% to 50% of patients and is a huge red flag for this specific disease.
You should also keep an eye on your nails. While people often think nail pitting or the nail lifting away from the bed (onycholysis) is just a cosmetic issue, it's actually a strong predictor of joint involvement. In fact, 80% to 90% of people with the arthritis version of the disease have nail changes, compared to much lower rates in those who only have skin psoriasis.
| Feature | Psoriatic Arthritis | Rheumatoid Arthritis |
|---|---|---|
| Joint Pattern | Often Asymmetric (Right hand, left knee) | Usually Symmetric (Both hands) |
| Skin Involvement | Common (Psoriasis patches) | Rare |
| Sausage Digits (Dactylitis) | Frequent | Very Rare |
| Blood Tests (RF) | Usually Negative (90% of cases) | Often Positive (70-80% of cases) |
The Different Ways It Hits the Body
Not everyone experiences this disease the same way. Depending on which parts of the immune system are most active, you might fall into one of a few patterns. Some people deal with symmetric polyarthritis, where many joints on both sides of the body are inflamed. Others experience asymmetric oligoarthritis, where only a few joints are affected, and they aren't mirrored on the other side of the body.
Then there is the spinal side of things. About 15% to 20% of patients develop spondylitis, which causes stiffness and pain in the vertebrae. In the most severe cases-affecting less than 5% of patients-arthritis mutilans can occur, leading to significant joint destruction. This is why getting a handle on the inflammation early is non-negotiable; untreated patients can see permanent joint damage within just two years.
Modern Treatment Paths
We've come a long way from just using creams and aspirin. The goal now is a "treat-to-target" approach, meaning doctors don't just want to make you feel "better," they want to bring your disease activity down to nearly zero to prevent permanent disability.
For many, the first line of defense involves DMARDs is Disease-Modifying Antirheumatic Drugs that slow down the progression of the disease . But for those who don't respond to standard pills, biologics have been a game-changer. These are engineered proteins that block specific parts of the immune system. TNF Inhibitors is a class of biologics like adalimumab or etanercept that target tumor necrosis factor to reduce inflammation . These are the heavy hitters that can clear skin patches and stop joint swelling simultaneously.
If you're looking for something newer, the FDA recently approved TYK2 inhibitors like deucravacitinib. These offer a different mechanism of action and can be a great alternative for people who didn't see results with traditional biologics. It's also worth noting that you'll likely need a TB test and a hepatitis panel before starting these, as they can suppress your immune system and make you more vulnerable to certain dormant infections.

Managing the Daily Grind
Medication is the foundation, but it's not the whole house. Dealing with the "brain fog" and crushing fatigue that 52% of patients report requires a lifestyle shift. Physical therapy is essential-not just to keep joints moving, but to strengthen the muscles around those joints to take the pressure off the inflammation.
You'll also want to build a "care team." Because this disease hits both the skin and the joints, you shouldn't just see one doctor. A coordinated effort between a rheumatologist (for the joints) and a dermatologist (for the skin) ensures that a drug treating your joints isn't accidentally making your scalp psoriasis worse, a phenomenon some patients have reported with certain medications.
Can I have the joint pain without the skin rash?
Yes. About 15% of people develop joint symptoms before any skin manifestations appear. If you have a family history of psoriasis but no rash, yet you're experiencing asymmetric joint swelling, you should still see a rheumatologist.
Is there a simple blood test to diagnose psoriatic arthritis?
Unfortunately, no. Unlike rheumatoid arthritis, which often shows a positive Rheumatoid Factor (RF), 90% of psoriatic arthritis patients are RF-negative. Diagnosis is usually based on a combination of clinical signs, like nail pitting and dactylitis, and your medical history.
Do biologics have side effects?
Yes, common ones include injection site reactions (reported by about 65% of users) and an increased risk of infections because the drug suppresses your immune system. This is why doctors require screening for tuberculosis before you start treatment.
How long does it take for treatment to work?
It varies. Some patients report a significant decrease in morning stiffness within 6 weeks of switching to a new biologic, while others may take 3 to 6 months to find the right dose and drug combination. Early intervention-within 12 weeks of onset-is key to preventing permanent damage.
Can diet help manage the inflammation?
While diet alone won't cure an autoimmune disease, reducing processed sugars and focusing on anti-inflammatory foods can help manage overall systemic inflammation and reduce the risk of cardiovascular comorbidities, which are more common in people with psoriatic arthritis.
Next Steps for Your Journey
If you're just starting to notice signs, don't wait. Start a symptom diary. Note when your joints are stiffest (usually the morning) and take photos of any skin changes or nail pitting. This data is gold for your doctor and can speed up a diagnosis process that otherwise takes an average of two years.
If you're already on a treatment plan but still feel "brain fog" or fatigue, talk to your specialist about adjusting your dosage or adding a physical therapist to your team. Remember, the goal is minimal disease activity, so if you're still struggling to get out of bed, your current treatment might need a tweak.